Medicine
The problem of metal
toxicosis associated with dental prosthetic constructions
*A.V. Pavlenko, Doctor of Medical Science, Professor, A.Yu. Nikonov, Cand. Sc. (Medicine),
Assistant Professor, O.V. Zaytseva, Doctor of Biological Sciences, Proessor,
M.A. Bondarenko, Cand. Sc. (Physics and
Mathematics), Assistant Professor, N.A. Gordienko, Cand. Sc. (Biology),
Assistant Professor
*National Medical Academy of Postgraduate Education named after P.D.
Shupik, Kyiv, Ukraine
Kharkiv National Medical University,
Kharkiv, Ukraine
Summary. Parametric and
nonparametric techniques, analyses of correlations, clusters and variance were
used in research of patients blood biochemical indices dynamics with
manifestations of metallic toxicosis by dentures before and after treatment. It
was detected clinical efficacy of tiotriazolin effect in comparison with
acetilcystein, and it has significant influence on blood biochemical indices of
AlATr, AsATr, MDA, CP (ceruloplasmin), total bilirubin. One may to consider tiotriazolin
as possible corrector of
oxidantic and antioxidantic homeostasis disturbances in metallic toxicosis in
orthopedic stomatology practice.
Key words: metallic
toxicosis by dentures; blood biochemical indices; statistical analysis;
tiotriazolin.
I. Introduction. Clinical observations and laboratory investigations have shown that
metal alloys used in prosthetic dentistry have significant systematic and local
effects [1-4]. The problem of metal toxicosis when using various metal
constructions of dental prostheses is still acute. Literature analysis and
internal investigations allow to suggest the imbalance between the
intensification of free radical oxidation in organism and the inhibition of
antioxidant system activity (depression of bioenergetic processes) being one of
the key factors in the patogenesis of metal toxicosis [5-8].
II. Objective setting. The objective of this project is to provide a statistical assessment of
the efficiency of prosthetic stomatopathy correction with Thiotriazolin.
There were 42 patients under observation showing
intolerance to titanium nitride coated stainless steel tooth prostheses. There
were 18 men and 24 women amongst the patients aged 27 to 45 years considering
themselves to be somatically healthy. The patients were divided into 2 groups
(n1=n2=21).
The clinical aspects of metal toxicosis fall within
the scope of three defined syndromes [10], determined as three severity levels.
After removal of fixed prostheses one group of the
patients was given medical treatment with a well-known, widely applied
medication Acetylcystein in doses of 0,6 g once a day and the other group with
an antioxidant and antihypoxant Thiotriazolin in doses of 0,1 g three times a
day during 21 days. Before and after the treatment the patients were examined
with a COBAS MIRA analyzer (Hoffmann-La Roche, Switzerland-Austria) for the
following biochemical blood values:
alanine aminotransferase and asparagine aminotransferase (ALT and AST)
activity; levels of total, direct and indirect bilirubin; concentrations of
serum ceruloplasmin (CP), transferrin (TF) and malone dialdehyde (MDA); levels
of sulfhydryl groups (-SH-).
These test values are meant to represent information
about the functionality of detoxifying organs such as liver, kidneys, spleen as
well as about the intensity of lipid peroxidation in organism and the activity
of antioxidant system.
The statistical analysis of the investigation findings
was performed using the Statistica 6.0 software package. The methods of
parametric and non-parametric statistics, correlation, cluster and dispersion
analysis were used [9].
III. Findings. In order to choose adequate analysis methods for the testing of the
effectiveness of Thiotriazolin in comparison with Acetylcystein basing on the
biochemical blood values in patients, the distribution laws of the examined
variables were studied first. For the normally distributed variables the
parametric methods were used, for those being not normally distributed the
non-parametric methods were applied. The inference about whether the
distribution law of each value is normal was made on the basis of the
Kolmogorov-Smirnov (K-S d) and Shapiro-Wilk (W) statistic values, Lilliefors
probabilities and their significance levels (p). It is found that such values as
ALT, AST and CP comply with the normal distribution law, whereas the
others are distributed not normally.
Prior to the main analysis, the groups of patients
given different medications were tested for homogeneity (as per their
biochemical values). For the normally distributed variables, Fisher’s analysis
(ANOVA) was applied, in case of the not normally distributed ones the
conclusion was made on the basis of the nonparametric Mann-Whitney and
Wald-Wolfowitz and two-sample Kolmogorov-Smirnov tests. The homogenous groups
were identified by cluster analysis. The descriptive statistics of the examined
values for two groups of patients are shown in Tables 1 and 2.
On the next stage, each group of patients given
different medications was tested for the dynamics of the biochemical values
before and after the treatment. The values before and after the treatment were
compared using the T-test for dependent samples, if normally distributed, and
its non-parametric equivalent, the Wilcoxon test, in case of an abnormal
distribution.
Table 1
Dynamics
of the biochemical values before and after the treatment with Acetylcystein.
Before the treatment:
|
Variable |
Descriptive Statistics
(result-1.sta) |
|||||||||
|
Valid N |
Mean |
Median |
Minimum |
Maximum |
Lower Quartile |
Upper Quartile |
Std.Dev. |
Standard Error |
||
|
AST |
20 |
0,73500 |
0,80000 |
0,30000 |
1,10000 |
0,60000 |
0,90000 |
0,236810 |
0,052952 |
|
|
Total bilirubin |
20 |
27,08500 |
27,20000 |
17,60000 |
43,30000 |
20,95000 |
30,65000 |
6,475645 |
1,447998 |
|
|
ALT |
20 |
0,91500 |
0,90000 |
0,50000 |
1,40000 |
0,75000 |
1,00000 |
0,256032 |
0,057251 |
|
|
MDA |
20 |
92,45500 |
94,05000 |
79,00000 |
100,00000 |
87,55000 |
98,15000 |
6,691194 |
1,496196 |
|
|
CP |
20 |
38,07000 |
38,30000 |
33,40000 |
40,50000 |
37,40000 |
39,50000 |
1,907078 |
0,426436 |
|
|
TF |
20 |
0,11850 |
0,12000 |
0,09000 |
0,14000 |
0,10000 |
0,13000 |
0,015313 |
0,003424 |
|
|
SH |
20 |
1,21000 |
1,20000 |
0,90000 |
1,40000 |
1,10000 |
1,35000 |
0,165116 |
0,036921 |
|
After the treatment:
|
Variable |
Descriptive Statistics
(result-1.sta) |
|||||||||
|
Valid N |
Mean |
Median |
Minimum |
Maximum |
Lower Quartile |
Upper Quartile |
Std.Dev. |
Standard Error |
||
|
AST |
20 |
0,63500 |
0,60000 |
0,20000 |
1,20000 |
0,50000 |
0,80000 |
0,245539 |
0,054904 |
|
|
Total bilirubin |
20 |
23,89500 |
23,50000 |
17,40000 |
37,50000 |
19,25000 |
26,05000 |
5,103814 |
1,141248 |
|
|
ALT |
20 |
0,76000 |
0,70000 |
0,40000 |
1,30000 |
0,60000 |
0,95000 |
0,268328 |
0,060000 |
|
|
MDA |
20 |
87,87000 |
90,25000 |
74,50000 |
97,20000 |
81,50000 |
92,10000 |
6,383457 |
1,427384 |
|
|
CP |
20 |
34,90000 |
34,70000 |
29,60000 |
41,50000 |
31,80000 |
38,10000 |
3,573882 |
0,799144 |
|
|
TF |
20 |
0,12050 |
0,12500 |
0,09000 |
0,15000 |
0,11000 |
0,13000 |
0,018771 |
0,004197 |
|
|
SH |
20 |
1,23000 |
1,25000 |
1,000000 |
1,40000 |
1,24444 |
1,30000 |
0,126074 |
0,028191 |
|
Table 2
Dynamics
of the biochemical values before and after the treatment with Thiotriazolin.
Before the treatment:
|
Variable |
Descriptive Statistics
(result-1.sta) |
|||||||||
|
Valid N |
Mean |
Median |
Minimum |
Maximum |
Lower Quartile |
Upper Quartile |
Std.Dev. |
Standard Error |
||
|
AST |
20 |
0,90500 |
0,90000 |
0,30000 |
1,40000 |
0,70000 |
1,10000 |
0,296426 |
0,066283 |
|
|
Total bilirubin |
20 |
23,88000 |
21,40000 |
17,60000 |
44,5000 |
19,50000 |
26,80000 |
6,584959 |
1,472442 |
|
|
ALT |
20 |
0,85500 |
0,90000 |
0,40000 |
1,3000 |
0,65000 |
1,00000 |
0,250210 |
0,055949 |
|
|
MDA |
20 |
89,52000 |
90,45000 |
76,40000 |
101,5000 |
81,75000 |
97,75000 |
8,775300 |
1,962217 |
|
|
CP |
20 |
38,04500 |
37,40000 |
33,40000 |
42,1000 |
36,35000 |
40,10000 |
2,320725 |
0,518930 |
|
|
TF |
20 |
0,11800 |
0,12000 |
0,09000 |
0,1400 |
0,11000 |
0,13000 |
0,014364 |
0,003212 |
|
|
SH |
20 |
1,20000 |
1,20000 |
0,90000 |
1,5000 |
1,00000 |
1,40000 |
0,194666 |
0,043529 |
|
After the treatment:
|
Variable |
Descriptive Statistics
(result-1.sta) |
|||||||||
|
Valid N |
Mean |
Median |
Minimum |
Maximum |
Lower Quartile |
Upper Quartile |
Std.Dev. |
Standard Error |
||
|
AST |
20 |
0 63500 |
0 70000 |
0,3000 |
0,90000 |
0,45000 |
0,80000 |
0,189945 |
0,042473 |
|
|
Total bilirubin |
20 |
18 42000 |
18,00000 |
14,0000 |
23,20000 |
17,15000 |
99,90000 |
2,039505 |
0,456047 |
|
|
ALT |
20 |
0 52000 |
0,50000 |
0,3000 |
0,90000 |
0,35000 |
0,60000 |
0,193581 |
0,043286 |
|
|
MDA |
20 |
75 13500 |
73,35000 |
69,50000 |
89,00000 |
71,5000 |
78,55000 |
5,484742 |
1,226426 |
|
|
CP |
20 |
28 85000 |
29,20000 |
24,20000 |
33,20000 |
26,95000 |
30,60000 |
2,552089 |
0,570664 |
|
|
TF |
20 |
0 12800 |
0,13000 |
0,09000 |
0,16000 |
0,11500 |
0,14000 |
0,020926 |
0,004679 |
|
|
SH |
20 |
1 29000 |
1,30000 |
0,90000 |
1,50000 |
1,20000 |
1,40000 |
0,171372 |
0,038320 |
|
The values before and after the treatment were compared using the
T-test for dependent samples, if normally distributed, and its non-parametric
equivalent, the Wilkoxon test, in case of an abnormal distribution.
Thus, in the 1st group of patients given
Acetylcystein the following values were found to be changed (decreased) after
the treatment: total bilirubin (р=0,000364), ALT (р=0,009563),
MDA (р=0,000120) and CP (р=0,002126). As an illustration, a bar chart is
presented for the CP value range before and after the treatment showing the
mean values of the variable, ± standard errors for the mean value and fiducial
limits (Figure 1).
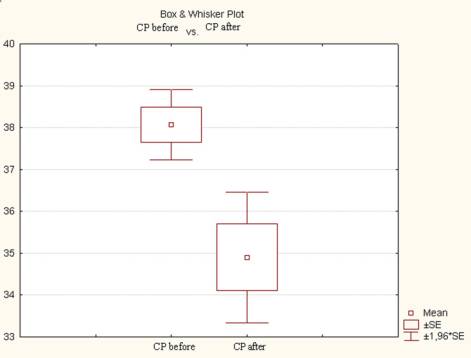
Fig.
1. CP variable value range before and
after the treatment in the 1st group of patients.
In the 2nd group of patients, where Thiotriazolin
was administered, the values changed (decreased) as follows: AST (р=0,000057),
total bilirubin (р=0,000219), ALT (р=0,000196), MDA (р=0,000089) and CP (р=0,000000).
The analysis of the obtained results shows that the treatment with
Thiotriazolin contributed to the reduction in the activity of the cytolytic
syndrome, i.e. in the activity of alanine and asparagine transaminase.
The bar charts in Figures 2 and 3 show the value
ranges for the AST, bilirubin, ALT and MDA variables before and after the
treatment in the 2nd group of patients.
The comparison of the efficiency of the treatment with
Acetylcystein and Thiotriazolin in two groups of patients involved the
determination of significant differences in the biochemical values after the
treatment. Upon completion of the treatment with these medications the two
groups showed significant differences in the following values: total bilirubin,
ALT, MDA, CP.
а)
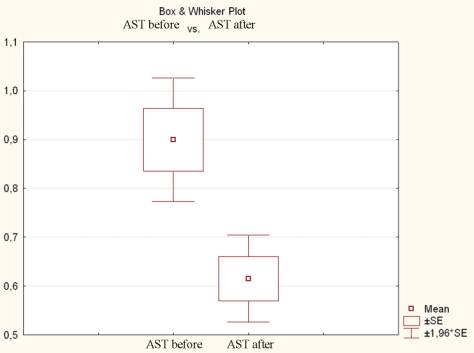
b)
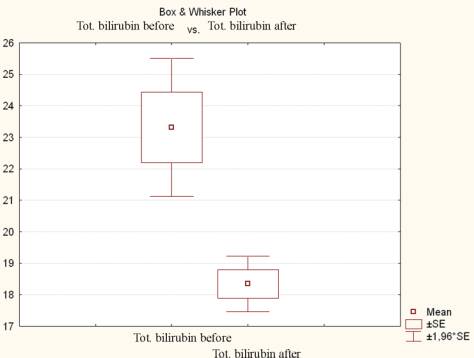
Fig.
2. Value ranges before and after the treatment in the 2nd group of
patients for the following variables: а) – AST; b) – bilirubin.
а)
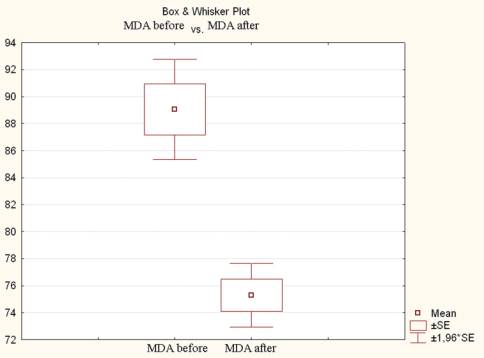
б)
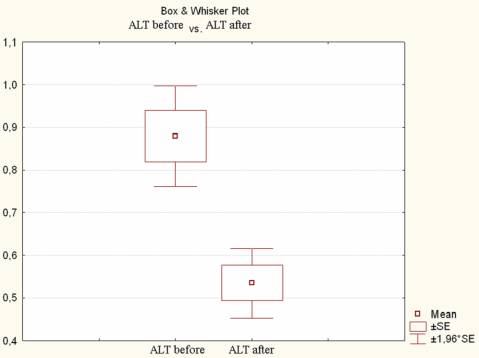
Fig.
3. Value ranges before and after the treatment in the 2nd group of
patients for the following variables: а)-MDA; b) – ALT.
The effectiveness of the treatment can be seen well in
the bar charts below showing the proportion of patients with different severity
levels before and after the treatment.
In Figures 4 and 5 the bar charts show the
redistribution of patients with different severity levels before and after the
treatment with both Acetylcystein and Thiotriazolin.
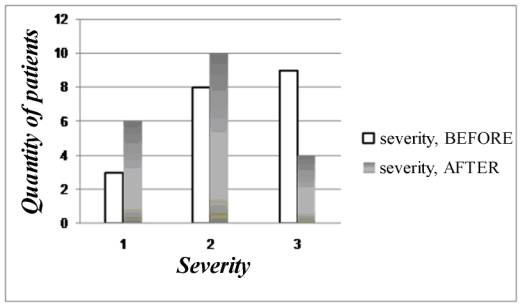
Fig
4. Severity levels within the 1st group of patients before and after
the treatment with Acetylcystein.
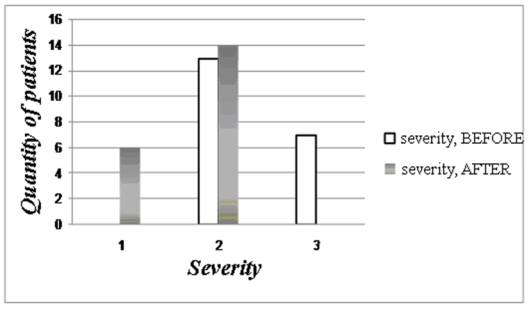
Fig
5. Severity levels within the 2nd group of patients before and after
the treatment with Thiotriazolin.
As we can see, the treatment with Acetylcystein has
led to a decrease in the number of patients with the third level of severity (9
before and 4 after the treatment), and an increase in the number of patients
with the lowest, the first severity level (3 before and 6 after the treatment).
The 2nd group consisted of patients with
the second and third levels of severity.
After the treatment with Thiotriazolin, the redistribution of patients
within the severity levels appeared to be more favorable as follows: there were
no patients with the third severity level at all, only patients with the second
and the first syndromes were observed.
IV. Conclusion. The analysis of the
dynamics of the biochemical blood values before and after the treatment in
patients with clinical symptoms of metal toxication caused by the use of dental
prosthetic constructions has shown that:
1.
The use of Thiotriazolin when curing prosthetic
stomatopathies, if compared with Acetylcystein, results in a more favorable
redistribution of patients within the severity levels. After the treatment with
Thiotriazolin, there were no patients observed with the third (the most
difficult) severity level, only patients with the first and second syndromes
were found out.
2.
Being a membrane protective agent with an
expressed antioxidant activity, Thiotriazolin appears to have more effect than
Acetylcystein on the level of such biochemical blood values as total bilirubin,
MDA, CP, as well on the activity of ALT and AST.
3.
It can be assumed that Thiotriazolin is one of
the potential medication for correction of the prooxidant-antioxidant homeostasis
known as the central factor in the pathogenesis of metal toxicosis in
prosthetic dentistry.
Further research in this field: studying the effect of
antioxidant nutrition in patients suffering from metal toxicosis caused by
fixed dental prostheses.
Literature
1. Гожий А.Г., Сагателян Г.Р., Гожая Л.Д.,
Большаков Г.В. Клинические проявления электрохимических процессов,
обусловленных отделочной обработкой зубных протезов из нержавеющей стали.
Стоматология 1998; 3 : 46-50.
2.Wirz J., Hermann J.S., Rateitschak–Pluss E.M. Причины непереносимости
зубных протезов. Клиническое наблюдение. Квинтэссенция 1999; 3: 19-26.
3.
Knoernschild K.L., Campbell S.D. Periodontal
tissue responses after insertion of artificial crowns and fixed partial
dentures. J. Prosthet. Dent. 2000; 5: 492-498.
4.
Salsano F., Francia C., Roumpedaki I. Immune
effect of nickel. Int. J. Immunopathol. Pharmacol. 2004; 17(2): 63-70.
5.
Никонов А.Ю. Нарушение
прооксидантно-антиоксидантного гомеостаза при введении никеля и нитрида титана.
Проблеми медичної науки та освіти 2005; 2: 49-52.
6.
Никонов
А.Ю. Биохимические изменения крови подопытных животных при введении в организм
никеля и нитрида титана. Вісник стоматології 2004;
4:11-14.
7.
Di Giampaolo L., Di Gioaccino M., Ponti J. “In
vitro” comparative immune effects of different titanium compounds. Int. J.
Immunopathol. Pharmacol. 2004; 17(2): 115-122.
8.
Ermolli M., Menne C., Pozzi G. Nickel, cobalt
and chromium – induced cytotoxicity and intracellular accumulation in human
hacat keratinocytes. Toxicol. 2001;15: 348-53.
9.
Ким
Дж.-О., Мюллер Ч.У., Клекка У.Р. и др. Факторный, дискриминантный и кластерный
анализ. Москва: Финансы и статистика, 1989. 215с.
10. Гожая
Л.Д. Аллергические заболевания в ортопедической стоматологии. Москва: Медицина,
1988:293 с.